
Ethics group calls for probe into Elon Musk's Neuralink brain implant
The group claims Musk made false statements about the safety of the device after several test monkeys died due to complications.
LEARN MOREAn experimental new device currently undergoing clinical trials may soon offer a safer, faster treatment for aneurysms.
Judy Sadler remembers when she found out about her brain aneurysm.
"I woke up in the morning at 3:00, had a bloody nose, checked my blood pressure, and it was over 200. And I thought, 'oh, brother.'
The 72-year-old says she's proactive about her health, and her symptoms — which also included severe headaches — were enough to see her doctor. Doctors did an MRI, and that's when they found the aneurysm — in between her eyes, in the front part of her brain.
"Just by chance," she recalls.
Sadler knew her father, mother, and sister each had an aneurysm around their lungs. Her doctor said those were caused by smoking. But this was different.
"Most times [brain aneurysms] are discovered kind of by accident, if you will," said Dr. Ian Kaminsky, neurointerventional surgeon at Swedish Medical Center near Denver, Colorado.
Kaminsky is part of a nationwide clinical trial currently testing a new device for treating wide-neck brain aneurysms — the type Judy Sadler had.
A brain aneurysm is a bulge coming off a weakened or injured part of an artery. The part between is called the "neck", and can be in various widths or shapes. You can think of the aneurysm like a balloon. It fills with blood. If it bursts, it can cause a stroke, brain damage, or even death. Surgery can be intense, requiring many tiny tools called stents and coils to block off the aneurysm. It can mean more medications too, and an increased risk of blood clots.
Kaminsky says wide-necks are among the more challenging, and depending on the size can take anywhere from 2 to 20 coils to block.
"Sometimes aneurysms have a very small opening or neck. In that case, it's easy to keep things like coils inside of them. But when an aneurysm has a wider opening, those devices tend to want to fall out into the parent blood vessel," he explains.
"The other option was to have two stents on either side of the blood vessels and a coil wiring inside. Well, I had a friend that had that, and it didn't do well," Sadler says.
The group claims Musk made false statements about the safety of the device after several test monkeys died due to complications.
LEARN MOREShe learned she was eligible for a new surgery, part of a nationwide clinical trial.
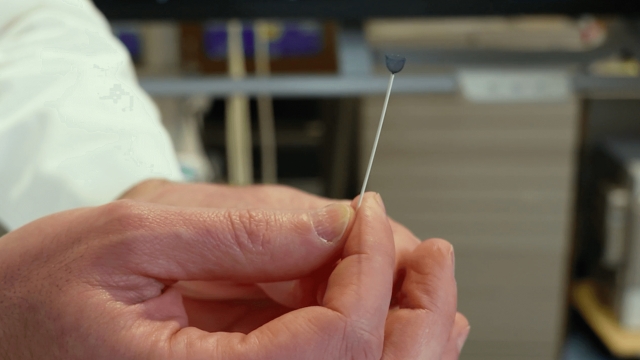
Her neurologist is on the same team as Kaminsky. Doctors would go in minimally and implant an experimental device shaped like a tiny straw that pushes out a flower-like cup that sits into the base of the wide-neck aneurysm, filling it.
"Basically, what you're doing is you're putting a catheter in the aneurysm, much like you would when you treat with coils. Except in this instance, you're putting in this one device that then shuts down the aneurysm," Kaminsky said.
It stops the blood from flowing in, meaning no bursting and very quick recovery time.
"You're not going to believe this. I went in at 5 a.m; 10 a.m. the next day, they released me. I was in the hospital for 30 hours. It was fabulous," Sadler says, giggling.
Sadler says she returned to work two days after coming home from the hospital after her March 21 procedure. She was back working part-time and volunteering within a matter of weeks. Some six months later, she's still doing well. She will follow up with doctors in March.
Roughly 1 in 50 people in the U.S. have an unruptured brain aneurysm. Every year there are about 30 thousand ruptured brain aneurysms — about one rupture every 18 minutes, according to the Brain Aneurysm Foundation.
There is another similar device that can be used and is already FDA approved. Kaminsky says it has a different cylindrical shape, and so surgeons may have a different preference.
Researchers across the country plan to study this device on at least 200 patients, and they are still enrolling them into the clinical trial. Kaminsky expects that should take a couple of years, and eventually, the device maker would move toward getting FDA approval.
COVID-19 continues to lead U.S. hospitalizations, the CDC says. Flu cases are climbing, and officials are hopeful RSV cases have now peaked.
Pfizer said its vaccine was 95% effective following its Phase 3 trial, but Texas' attorney general said the data was too premature.
Dr. Mona Hanna-Attisha, a pediatrician and whistleblower who dealt with the water crisis in Flint, Michigan, says the plan will help protect kids.
40% of engagements take place between Thanksgiving and Valentine's Day, according to industry experts.
CBP officials say the Tucson area, including Nogales, is already seeing the highest number of migrants coming into the country.
25 million U.S. students use diesel-powered school buses daily, prompting debates on cleaner alternatives.
